
Who Will See Me Now?
The doctor will see you now.
The nurse practitioner will see you now.
The physician assistant will see you now.
The provider will see you now.
We have sold our souls my friends. In our eagerness to hand over control of hospitals, we have turned medicine into a commodity easily bartered, bought and sold to the lowest bidder. Physicians, nurses and patients have become incorporated into the larger industrial complex previously known as health care. We have been determined to be replaceable cogs. Lose a veteran 20-year physician, replace it with a cheaper physician assistant and call them a provider.
In areas where care can be streamlined and made more efficient, with minimal interruptions make it so.
As a physician. I was amazed and appalled at the process when I stepped into the patient gown.
Now I’m the patient
In September of 2022, I received an automated notice from my healthcare organization that it was time for my colonoscopy. My primary care physician (PCP) was out until March 2023. I tried to locate my colonoscopy report from years past to find out why. Alas, it was not in the record. I called my gastroenterologist (GI) who, with 4-follow up phone calls, was eager to schedule my appointment with first availability in January 2023. Five months out. Yeesh. Okay.

My prescription was sent to the pharmacy 5 months ahead of time. As were the list of instructions. When I had questions later about downtime following the procedure and whether flying was limited, it took multiple phone messages as there was no way to message the GI doctor directly.
My question was eventually answered. I get it. I would not want to have to answer a multitude of questions if my scheduling team or nurse could.
The day of the event. It was the smoothest, slickest procedure ever, but I couldn’t help but feel like I was going down a conveyor belt. They had optimally timed the event from arrival to departure. Each person had a specific role and knew it well.
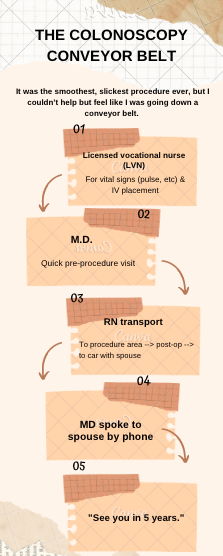
It felt quite impersonal. No discussion about methods of mitigating my risk for colon cancer. Just see you in five years. And I can bet you that this is because health insurers pay much more in RVUs (resource value units) for the procedure itself than for a discussion of diet and lifestyle changes to optimize your health.
Patients want information
Patients are hungry for information: well-curated, researched and easy-to-understand information. Alas, physicians are too busy getting pre-authorizations, documenting new CMS (Centers for Medicare & Medicaid Services) criteria and hiring additional staff as the great exodus from health care continues. And patients aren’t happy. And rather than hire another middle manager to explore the reasons that patients aren’t happy, it is time for us to admit our culpability in this debacle as we raced to maintain our patients per hour to maximize our dollars home.
And what happened, American Medical Association?
Have you sold your souls too? Nary a ripple of complaint as the American Association of Nurse Anesthetists changed their name to the American Association of Nurse Anesthesiologists, so now they can say I am an anesthesiologist. Nurses who completed a research project while getting their Nurse Practitioner’s degree can say that they are a doctor? The healthcare system is misleading patients. That is not acceptable.
Back to Malcolm Gladwell’s 10,000 hours, physician assistants, nurse practitioners, and physicians all play important roles in the health of patients. However, it is dangerous to equate the level of training of all 3 by referring to all of them as doctors or providers.
How would a lawyer feel if a paralegal argued in court using false information and the lawyer who was not present was found liable, and the lawyer was sued or potentially disbarred. It would not happen. Why have we allowed this to happen in medicine? Why can physician assistants and nurse practitioners be allowed to practice independently with “physician oversight”? Physician oversight being a perusal of the chart 1-2 weeks later.
Disclaimer
The information in this blog is provided as an information and educational resource only. It is not to be used or relied upon for diagnostic or treatment purposes.
The blog does not represent or guarantee that its information is applicable to a specific patient’s care or treatment. The educational content in this blog is not to be interpreted as medical advice from any of the authors or contributors. It is not to be used as a substitute for treatment or advice from a practicing physician or other healthcare professional.




